Global prevalence of occult hepatitis B: a systematic review and meta-analysis
Hepatitis B (HepB) is an international public health challenge that can lead to progressive scarring in hepatocellular carcinoma and primary liver cancer, and accounts for a significant proportion of viral hepatitis. The World Health Organization estimates that 296 million people were living with chronic hepatitis B infection in 2019, with about 820,000 deaths. About 90 million people in China suffer from chronic hepatitis B, and an estimated total of 300,000 die of hepatitis B-related diseases every year[1].
Occult/undiagnosed HBV infection (OBI) is defined as the presence of replication-competent HBV DNA in the serum of individuals who are negative for liver and/or HepB surface antigen (HBsAg). Stability and persistence of HBV cccDNA in the nucleus of hepatocytes are the molecular basis of occult HepB infection (OBI). OBI can be transmitted through blood transfusions or organ transplants. And receiving chemotherapeutic agents or other immunosuppressive agents may trigger reactivation of HBV replication in individuals with OBI. Therefore, it is crucial to assess the prevalence of OBI. Studies have shown that there are significant differences in the prevalence of OBI in different populations worldwide. However, no data are available on the prevalence of OBI in the global population.
The First Affiliated Hospital of Nanjing Medical University, in collaboration with the Wright Center for Graduate Medical Education in Scranton, Pennsylvania, USA, published an article days ago in the Journal of Viral Hepatitis: Global prevalence of occult Hepatitis B: a systematic review and meta-analysis, providing a description of the global prevalence of OBI and other relevant content through systematic search of data and meta-analysis.
During the period from database creation to December 27, 2018, the study searched for relevant articles in PubMed, Embase, CINAHL, Cochrane, and Web of Science, and a total 98 papers on the prevalence of OBI from 34 countries and regions were finally included after an initial screening of 2325 records. The major results are summarized as follows:
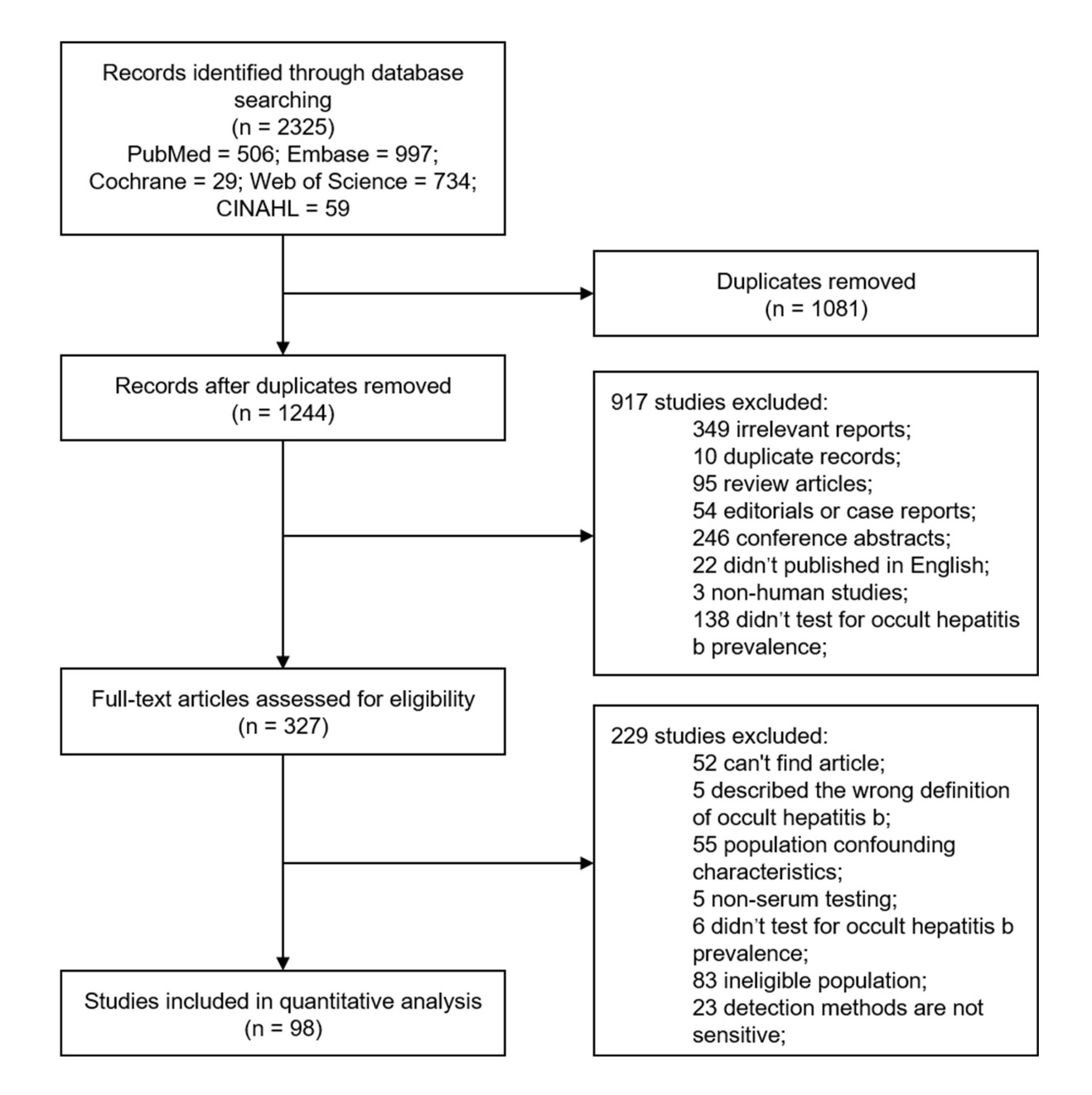
1. Data selection process
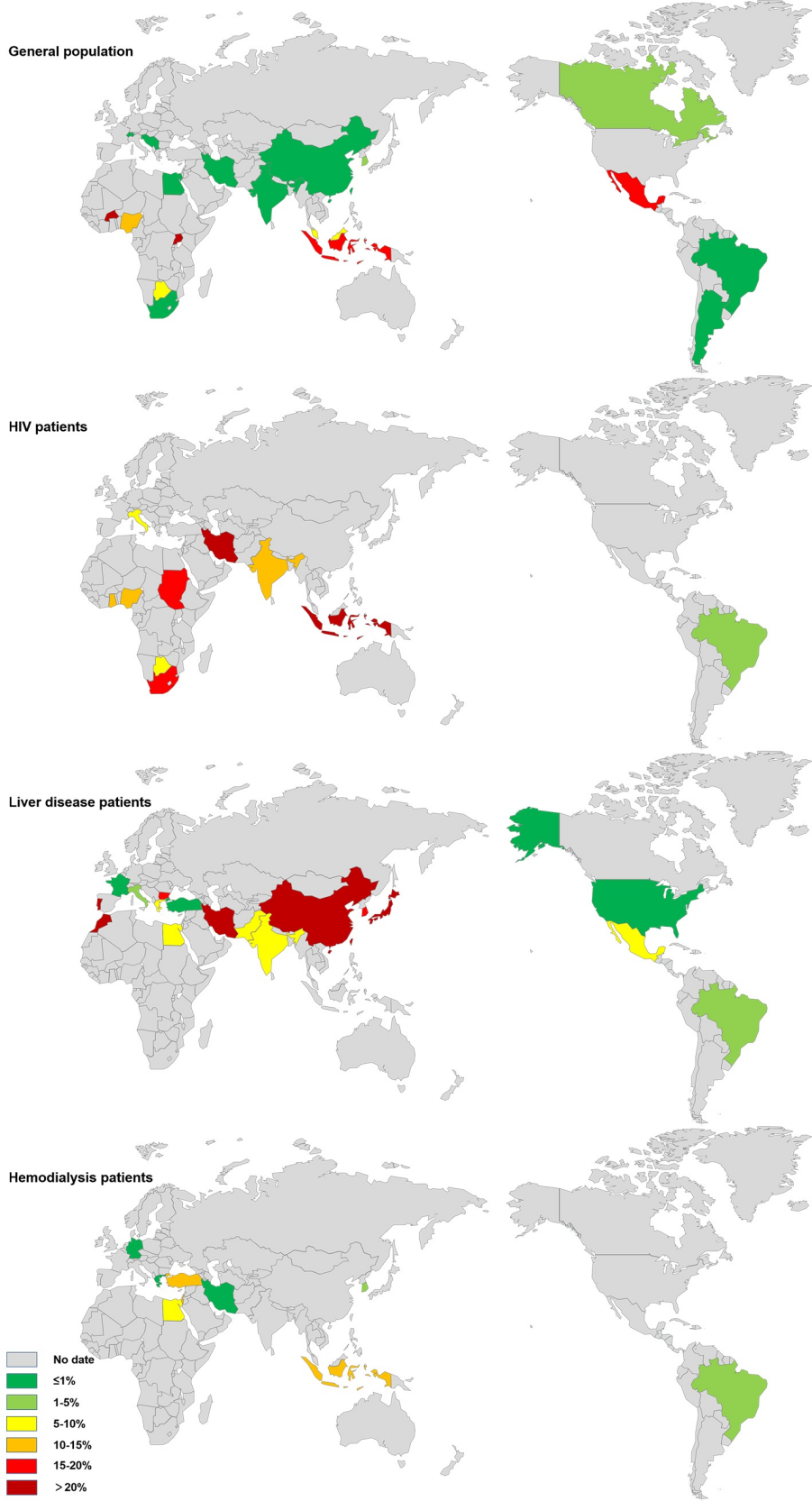
A total of 2325 records were searched in the relevant database using the keywords “occult hepatitis b infection” and “prevalence”, and 98 studies remained after removing duplicates and ineligible ones. There were 114 cohorts from 34 countries and regions with a total of 3,681,117 individuals that made up the final cohort. The 114 cohorts included 45 cohorts (3667171) of general population, 15 cohorts (3801) of HIV carriers, 27 cohorts of (4074) of patients with liver disease, 14 cohorts (2694) of hemodialysis (HD) patients, and 13 cohorts (3377) of those with other risk factors.
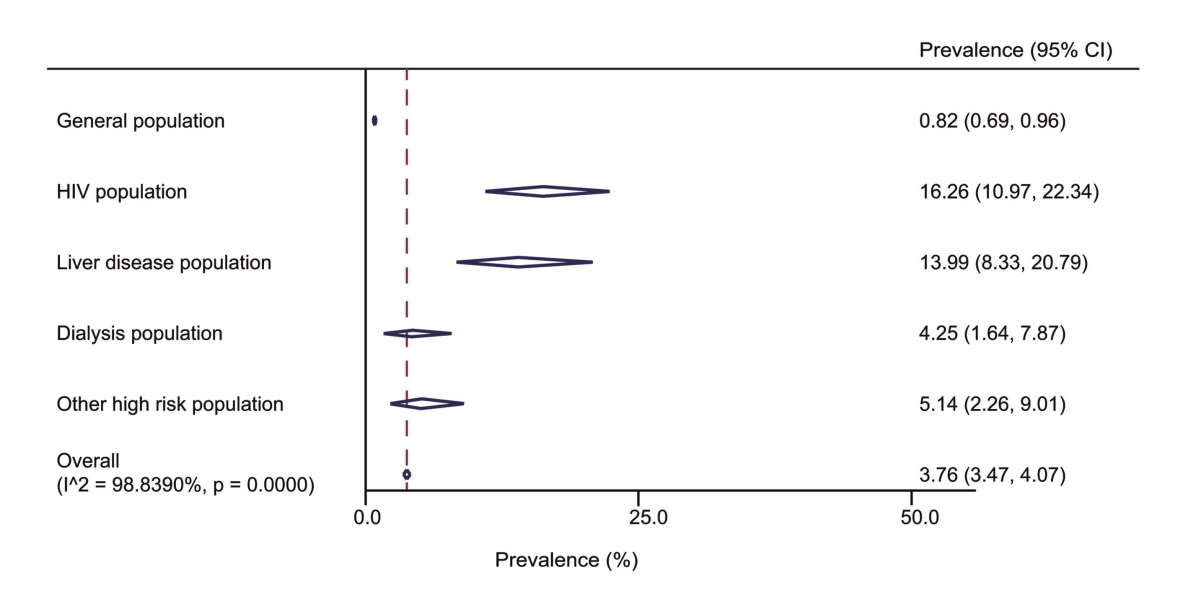
2. Meta-analysis of occult hepatitis B infection rates in different populations
Data analysis by the team showed significant differences in the prevalence of OBI among the four high-risk groups. The prevalence of OBI was 16.26% (95%CI 10.97 – 22.34) in HIV patients, 13.99% (95%CI 8.33 – 20.79) in patients with liver disease, 4.25% (95%CI 1.64 – 7.87) in hemodialysis patients, and 5.14% in those with other risk factors (95%CI 2.26 – 9.01). The results suggested that OBI was highest prevalent in the HIV population, but lowest in hemodialysis patients. And the 4 high-risk groups had a significantly higher prevalence than the general population (0.82%).
3. Meta-analysis of OBI infection rates in the general population at different socio-demographic index (SDI) levels
The Socio-Demographic Index (SDI) is a combination of factors including GDP per capita, the average number of years of schooling for adults and the fertility rate for women under the age of 25. Simply put, the SDI involves an overall assessment of the level of development of a country or region.
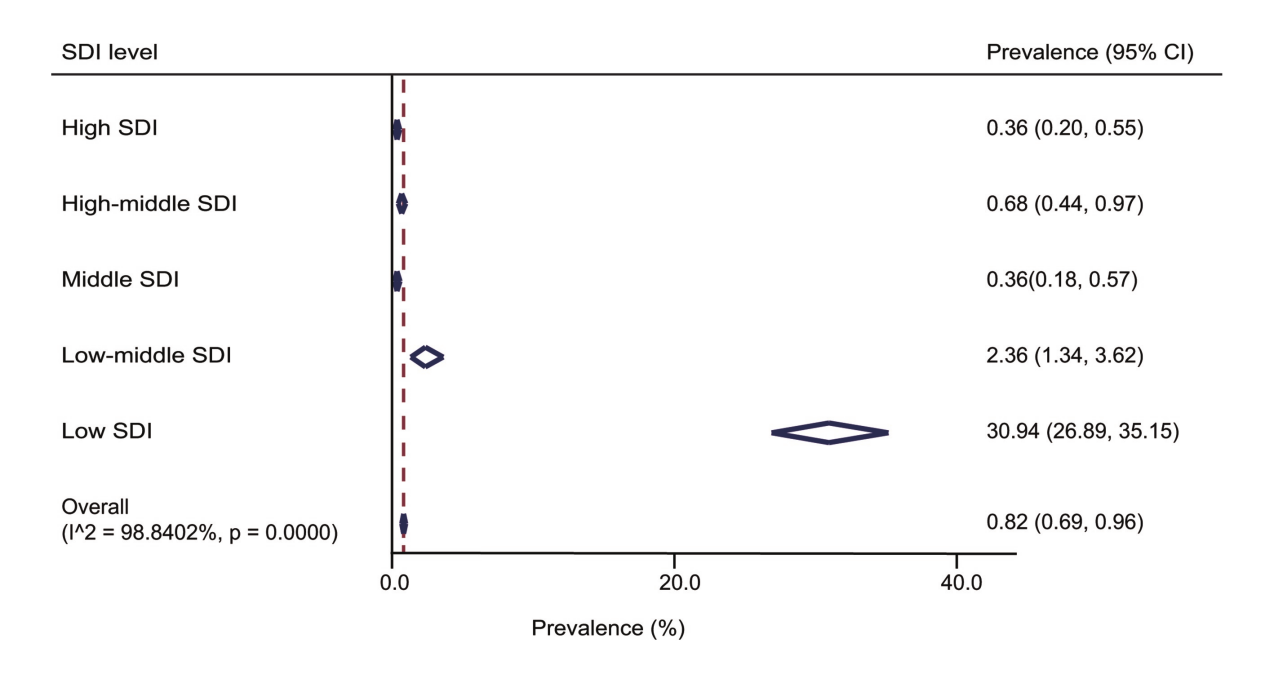
The previous analysis showed that the prevalence of OBI in the general population was 0.82% (95%CI 0.69 – 0.96). For the general population, the prevalence of OBI also varies considerably across countries with different SDI levels. The prevalence of OBI was 0.36% (95% CI 0.20-0.55) in countries with high SDI, 0.68% (95% CI 0.44 – 0.97) in countries with moderate to high SDI, 0.36% (95% CI 0.18 – 0.57) in countries with moderate SDI, 2.36% (95% CI 1.34-3.62) in countries with moderate to low SDI, and 30.94%(95% CI 26.89-35.15) in countries with low SDI. As expected, the countries with the highest prevalence of OBI were those with low SDI and vice versa.
4. Meta-analysis of the prevalence of occult hepatitis B infection in the general population at different HBV prevalence levels
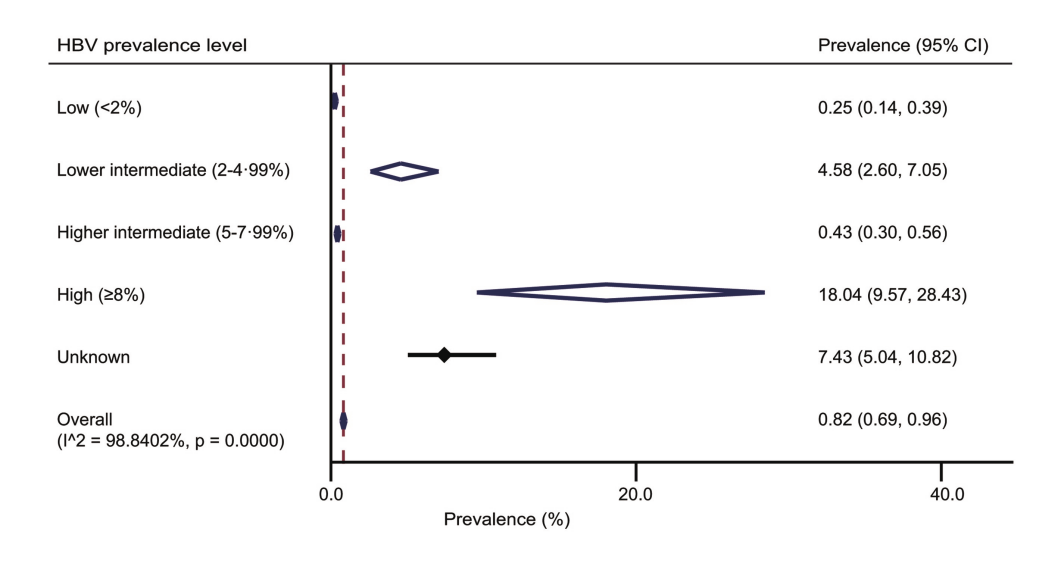
The study went on to analyze the prevalence of occult hepatitis B in the general population at different HBV prevalence levels. The prevalence of OBI was 0.25% (95% CI 0.14-0.39) in populations at low HBV prevalence levels, 4.58% (95% CI 2.60 – 7.05) in populations at relatively low HBV prevalence levels, 0.43% (95% CI 0.30 – 0.56) in populations at relatively high HBV prevalence levels, and 18.04% (95% CI 9.57 – 28.43) in populations at high HBV prevalence levels. The results suggested that the prevalence of OBI was significantly higher in populations at high prevalence levels of hepatitis B than in those at low prevalence levels.
Conclusions
Studies have found that immune deficiencies in HIV-infected patients make OBI and HBV reactivation more likely to occur. Therefore, HBV DNA testing is recommended for screening and identification of OBI in HIV-positive patients. Hemodialysis patients are considered to be in an immunosuppressed state and exposed to a variety of invasive procedures. Patients with OBI may be at risk of nosocomial transmission during hemodialysis treatment, so hepatitis B vaccination, screening of blood and blood products, and infection control measures are recommended as means of preventing hepatitis B transmission.
The underlying mechanism of OBI is still unknown. It is believed to be primarily due to the strong inhibition of viral replication and gene expression, which may also involve wild-type strains. A cure for HBV (elimination of HBV) may not be achievable as HBV DNA is integrated into the host genome. Therefore, close monitoring is needed to identify HBV reactivation, especially in patients receiving chemotherapeutics or other immunosuppressive treatments and in patients with acquired immune deficiency syndrome. The clinical significance and virological/immunological mechanisms of OBI still remain controversial, and reliable epidemiologic data need to be collected to help countries determine OBI prevalence and guide their prevention and management policies.
Finally, the results of this study emphasized the need for clinical diagnosis of OBI. HBV DNA testing methods need to be standardized to facilitate investigation of the reliability of HBV antibody and DNA testing worldwide. Since the incidence of OBI in special populations (HIV, liver disease and hemodialysis patients) is significantly higher than in the general population, clinical diagnosis of OBI and screening are quite essential. OBI can be transmitted through blood. Current infectious disease screening strategies based on immunology have the possibility of missing OBI detection, and supplemental nucleic acid screening for hospitalized and physical examination population, especially the high-incidence population, enables early detection and clinical diagnosis and timely treatment, while reducing the risk of hospital cross-infection, and preventing health care infection and unnecessary medical disputes.
References:
1. ESansure (2022-03-11): The Lancet – The need for and cost effectiveness of universal hepatitis B screening in China
2. Ji DZ, Pang XY, Shen DT, Liu SN, Goyal H, Xu HG. Global prevalence of occult hepatitis B: A systematic review and meta-analysis. J Viral Hepat. 2022 May;29(5):317-329. doi: 10.1111/jvh.13660. Epub 2022 Mar 12. PMID: 35253969.
Note: The picture comes from the Internet. If there is any infringement, please contact the author to delete it.
Disclaimer: All the publications on this website, where the source is indicated, are copyrighted by the original source and do not represent the position of this website.



{kind=link}